Health
UN: World Eating Too Much Sugar; Cut to 5-10 Percent of Diet

In this Dec. 18, 2001 file photo, an orange juice company employee works at a plant in Cuautitlan, Mexico. New guidelines published by the World Health Organization on Wednesday, March 4, 2015 say the world is eating too much sugar and people should slash their sugar intake to just 5 to 10 percent of their overall calories. (AP Photo/Marco Ugarte, File)
MARIA CHENG, AP Medical Writer
LONDON (AP) — New guidelines from the World Health Organization are enough to kill anyone’s sugar high. The U.N. health agency says the world is eating too much sugar and people should slash their intake to just six to 12 teaspoons per day — an amount that could be exceeded with a single can of soda.
So, put down that doughnut. And while you’re at it, skip the breakfast cereal, fruit juice, beer and ketchup.

The guidelines, released Wednesday, finalize draft advice first released last year and are focused on the added sugars in processed food, as well as those in honey, syrups and fruit juices. The advice does not apply to naturally occurring sugars in fruit, vegetables and milk, since those come with essential nutrients.
“We have solid evidence that keeping intake of (added) sugars to less than 10 percent of total energy intake reduces the risk of overweight, obesity and tooth decay,” Francesco Branca, director of WHO’s nutrition department, said in a statement.
Experts have long railed about the dangers of sugar and studies suggest that people who eat large amounts of the sweet stuff are at higher risk of dying prematurely from heart problems, diabetes and cancer, among other conditions.
To meet the lower threshold set by the new guidelines, Americans, Europeans and others in the West would have to slash their average sugar intake by about two-thirds.
Americans get about 13 percent of their calories from added sugar, or 268 calories a day, the equivalent of about 18 teaspoons. One teaspoon of sugar is about 15 calories. In Europe, sugar intake ranges from about 7 percent in Hungary and Norway, to 17 percent in Britain to nearly 25 percent in Portugal.
Some experts said the 10 percent target was more realistic for Western countries than the lower target. They said the 5 percent of daily calories figure was aimed mostly at developing countries, where dental hygiene isn’t good enough to prevent cavities, which can lead to serious health problems.
Last month, a U.S. government advisory committee recommended that sugar be limited to 10 percent of daily calories, marking the first time the U.S. has called for a limit on added sugars. The Agriculture and Health and Human Services departments will take those recommendations into account when writing the final guidelines, due by the end of the year.
WHO had previously suggested an upper limit for sugar consumption of around 10 percent, but issued the 5 percent guidance based on the presumed additional health benefits from cutting intake even further, though it said it had no solid evidence to support that.
“To get down to 5 percent, you wouldn’t even be allowed to have orange juice,” said Tom Sanders, a professor of nutrition and dietetics at King’s College London who wasn’t part of the WHO guidelines.
He said it shouldn’t be that difficult for most Europeans, Americans and others in the developed world to get their sugar intake to 10 percent of their diet if they limit things like sugary drinks, cereals, beer, cookies and candy.
“Cake is lovely, but it’s a treat,” Sanders said.
The Sugar Association slammed the new recommendations, arguing the advice was based on “poor quality, weak and inconsistent data.” It noted WHO itself acknowledged the evidence for the 5 percent target was “very low quality.”
The International Council of Beverages Associations echoed those concerns and said beverage makers can help people cut back on sugar through smaller portion sizes, as well as no- and low-calorie drinks and providing nutritional information on labels.
Coca-Cola, for example, has been more aggressively marketing its “mini cans” and has launched a reduced-calorie version of its namesake soda called Coca-Cola Life that’s sweetened with a mix of sugar and stevia, a natural sweetener. Companies have also been working on new technologies to reduce sugar. Senomyx, based in California, makes ingredients that interact with taste receptors to block or amplify sweetness. They have no taste or smell and are listed as artificial flavors.
Last year, the U.S. proposed new nutrition labels that would be required to list any sugars added by manufacturers.
Sugar is just one of a number of ingredients that have come under attack, such as salt and trans fat. However, WHO pointed out that when it comes to sugar, most people don’t realize how much they’re eating because it’s often hidden in processed foods not considered sweet. For example, one tablespoon of ketchup has about 4 grams (1 teaspoon) of sugar and a single can of soda has up to 40 grams (10 teaspoons).
“The trouble is, we really do like sugar in a lot of things,” said Kieran Clarke of the University of Oxford, who said the global taste for sugar bordered on an addiction. “Even if you are not just eating lollies and candy, you are probably eating a fair amount of sugar.”
Clarke noted that there’s added sugar even in pasta sauces and bran cereals. She said fruit juices and smoothies were common dietary offenders, because they have very concentrated amounts of sugar without the fiber benefits that come with eating the actual fruit.
Clarke welcomed the new WHO guidelines but said people should also consider getting more exercise to balance out their sweet tooths.
“If you do enough exercise, you can eat almost anything,” she said. “But it’s very hard to avoid large amounts of sugar unless all you’re eating is fruits and vegetables.”
___
Associated Press writers Candice Choi in New York and Mary Clare Jalonick in Washington contributed to this report.
___
Online:
WHO’s sugar guidelines
http://apps.who.int/iris/bitstream/10665/149782/1/9789241549028_eng.pdf
Copyright 2015 The Associated Press. All rights reserved. This material may not be published, broadcast, rewritten or redistributed.









Commentary
Standing Room Only in Raleigh with Leader Sydney Batch and Stacey Abrams
THE CAROLINIAN — North Carolina Senate Democratic Leader Sydney Batch and national voting rights champion Stacey Abrams held a data-driven discussion in Raleigh on critical policy issues facing North Carolina and the nation. The event, framed as a Jeopardy-themed fundraiser, explored topics such as systemic healthcare failures and threats to the judiciary and voting infrastructure.

By Jheri Hardaway, Staff Writer | The Carolinian
Raleigh, NC — It was a standing-room-only crowd in Raleigh as North Carolina Senate Democratic Leader Sydney Batch took the stage alongside national voting rights champion, attorney, and author Stacey Abrams for an intensive, data-driven Jeopardy-themed conversation on the political landscape. Way more innovative than standard campaign events, the fundraiser served as an evidence-based dissection of the most critical policy issues facing North Carolina and the nation, from structural failures in the healthcare system to coordinated threats against the judiciary and voting infrastructure.
The forum underscored a singular theme: true leadership does not distort the facts for comfort; it empowers communities by confronting brutal truths with an actionable strategy for progress. The evening kicked off with audience members selecting policy categories to guide the discussion. The first critical issue raised concerned the North Carolina State Health Plan and the state’s obligation to provide affordable, accessible healthcare to public employees and retirees without shifting the burden to them through increased premiums and co-pays.
Leader Batch addressed the crisis directly, pointing to fifteen years of fiscal management under opposing legislative leadership that failed to protect the state’s infrastructure. “We waited over a decade to have Medicaid expansion,” Batch stated, drawing a direct line between systemic policy delays and rising costs for private policyholders. “It isn’t about the fact that it’s going to just go down because all of a sudden we remove people from the rolls. All of us with private insurance are going to continue to pay the price because the uninsured are the most vulnerable.”

Batch, a cancer survivor who received treatment at UNC, shared a profound personal perspective on the geographic disparities embedded in the healthcare system, noting she met patients traveling from Nash County and the coast because vast swathes of North Carolina have become medical deserts.
The policy conversation grew sharper when analyzing the raw data of the current state budget. Batch highlighted the stark economic reality of a state maintaining a minimum wage of $7.25 an hour, amounting to just $15,080 a year for an individual working 40 hours a week for 52 weeks without a single day off. Despite this, she noted, the legislature’s current budgetary trajectory imposes higher co-pays and premiums on the expansion population and state employees.
Stacey Abrams echoed these concerns by providing data from Georgia, a state that spent $80 million on a partial Medicaid expansion model, two-thirds of which was swallowed by administrative costs rather than direct patient care. “Medicaid expansion is life-saving care,” Abrams urged, noting that Georgia’s refusal to fully expand Medicaid has left it with some of the worst maternal mortality rates in the nation and led to the systemic closure of rural and metropolitan hospitals alike.
In North Carolina, Batch noted that while progress has been made, such as extending postpartum Medicaid coverage for pregnant women from 60 days to 12 months. New hurdles, such as retrogressive three-month lookback periods and complex work requirements, threaten to deter families from seeking care. “When you are turned down once, you are unlikely to ever sign up again,” Batch warned. “That is not going to reduce the cost of medical care and treatment; it’s only going to increase it.”
The dialogue shifted to the legal and community protections necessary to combat stringent voting laws, including the strategic removal of polling places from historically Black colleges and universities (HBCUs) and minority communities. When asked what concrete measures can prevent voter intimidation at the ballot box, Leader Batch called for radical civic participation and the deployment of human infrastructure. She recalled past election cycles where voters in her own district faced intimidating displays, including oversized Confederate flags and armed individuals at polling sites. Batch emphasized the necessity of trained, nonpartisan observers and volunteer attorneys. “What we need to do as a people, and so many of you in this room with privilege need to do, is be there at these polling places,” Batch asserted. “You need to be those nonpartisan observers. You need to be the line that holds… We are doing our very best to make sure that we are hiring and we have a lot of volunteer attorneys to be on this line.”
Abrams contextualized this fight by emphasizing the practical, block-by-block mechanics of election security. “Help people make a plan to vote, make certain they know what day the election is,” Abrams advised, reminding the audience that working-class voters often carry logistical burdens that obscure election timelines. “We owe it to our ancestors. They’ve been through worse. So now it’s our turn.”
A central focus of the evening was a granular breakdown of what it takes to break the legislative supermajority in North Carolina and protect the judiciary from hyperpartisan overreach. The financial and strategic calculus laid out by Leader Batch presented a compelling argument for the efficiency of investing in state legislative races:
The U.S. Senate Math: A competitive, top-of-the-ticket statewide race in North Carolina can easily command a staggering $800 million in collective spending.
The NC Senate Math: By contrast, the entire Senate Democratic Caucus can mount a highly competitive battle to build a working majority for roughly $12 million.
“That is 1.5% of the entire U.S. Senate spend,” Batch calculated, demonstrating how direct financial resources go significantly further in targeted local legislative districts. To break the current Republican supermajority, the Senate Democratic Caucus needs to net just one seat to reach 21, while a “great year” could push the caucus to 23 or 25 seats, securing a functional tiebreaker alongside the executive branch.
Abrams backed this strategy by pointing to historical data from her 2018 gubernatorial run in Georgia. While she narrowly missed the executive mark by 53,794 votes, the targeted, down-ballot investment successfully flipped 14 legislative seats and broke a devastating supermajority. “All of the evil that they do that they cannot get through an impotent Congress is coming to a state near you,” Abrams warned, framing state legislatures as the primary battlegrounds for modern policy warfare.
Furthermore, both leaders stressed that legislative majorities are the ultimate defense mechanism for the judiciary. Batch raised the alarm regarding partisan maneuvers across the country, such as the introduction of recall mechanisms targeting independent judiciaries, and warned that maintaining seats like Justice Anita Earls’ on the North Carolina Supreme Court is crucial to preventing the systematic dismantling of democratic oversight.
Closing the night under the banner of “Keeping Hope Alive,” Abrams shifted the perspective from defensive posturing to a proactive framework for civic engagement. She contrasted the mechanics of authoritarianism, which she defined as taking power, hoarding power, and avoiding accountability. Democracy, which requires sharing power, leveraging power for the collective benefit, and maintaining strict accountability. Abrams challenged the audience to push back against the weaponization of language, specifically the targeted attacks on Diversity, Equity, and Inclusion (DEI) frameworks. “They see DEI for what it is: Diversity is people, Equity means fair access to opportunity, and Inclusion means respect for belonging,” Abrams declared. “In a democracy, that’s the DNA… We can’t let them seize our language and scare us into not calling the truth out. When they do that, we lose. When we refuse to let them take our language, we win.”
To counter structural voter fatigue, Abrams directed attendees to the 10 Steps Campaign, an action-oriented initiative designed to provide everyday citizens with an explicit plan for local resistance. The strategy hinges on executing practical steps: hosting and sharing informational narratives, organizing locally, litigating in both the courts and the court of public opinion, utilizing nonviolent disruption, and consistently engaging elected officials up and down the ballot.
As the standing-room crowd dispersed, the mandates left behind by both leaders were clear: fundraising is not merely an aggregation of dollars, and democracy is not a passive experiment. It is a continuous, disciplined application of hope, labor, and strategy.
Based on reporting by The Carolinian.
Commentary
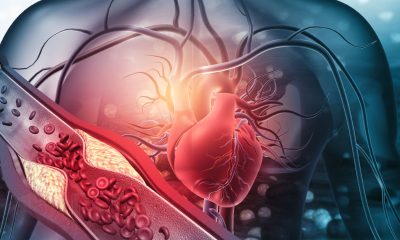
Preventing Amputation: A Doctor’s Guide for Diabetes Patients
POST NEWS GROUP — Amputation is usually the final stage of diabetic foot disease. Earlier signs often involve nerve damage. Some people experience numbness, tingling, burning, or loss of sensation in their feet.

For many diabetes patients, amputation becomes a last-resort measure after infections, ulcers, or poor circulation worsen rapidly and leave few other treatment options.
But according to Dr. Estelle Everett, a physician and researcher specializing in endocrinology, diabetes, and metabolism at the
University of California Los Angeles (UCLA), most diabetes-related amputations can be prevented through early intervention, consistent medical care, and patient education.
For Everett, her commitment to diabetes prevention is deeply personal. Watching her younger sister navigate Type 1 diabetes exposed her early to the challenges many patients face, including barriers to advanced diabetes technologies such as continuous glucose monitors and insulin pumps due to racial disparities in patient care.
Those experiences helped shape her focus on prevention, education, and equitable access to care.
Dr. Everett spoke with California Black Media (CBM) about the warning signs of diabetic complications, prevention strategies, healthcare access, and the role of diabetes technology in improving outcomes.
What are some of the early warning signs that a person with diabetes may be developing circulation and nerve problems that could potentially lead to amputation?
Amputation is usually the final stage of diabetic foot disease. Earlier signs often involve nerve damage. Some people experience numbness, tingling, burning, or loss of sensation in their feet.
Poor circulation is another warning sign. Symptoms can include calf pain while walking, foot pain at rest, cold feet, skin color changes, or wounds that do not heal properly. Foot ulcers, thick calluses, and untreated cuts can also become serious infections that may eventually lead to amputation if they are not treated early.
Before complications reach that stage, what are some early signs of diabetes itself that people should be looking out for?
Many people are walking around with diabetes and do not even realize it. Some patients first seek medical care only after they’ve already developed complications because they’ve had diabetes for years without knowing it.
That’s why routine screenings are so important. If you have diabetes, controlling it early can significantly reduce the risk of severe complications later on.
Many Black Californians harbor a degree of distrust in the healthcare system. What message would you send to encourage people to get regular checkups?
Distrust is real, and there are many reasons people may avoid healthcare. Some fear discrimination or worry they’ll simply be judged instead of helped.
Personally, I realized some of the care my sister received may have been influenced by racial bias. Although she had diabetes for years, she was never offered diabetes technology like insulin pumps or continuous glucose monitors. When she finally asked about them, she was told she had to jump through many hoops.
Later, I realized her experience wasn’t unique. Research shows that minority patients and people from lower-income backgrounds are less likely to be offered diabetes technology. That inspired me to focus my research on improving access for the populations that need these tools the most.
I think building trust is important. Finding the right doctor is almost like dating. If you don’t feel comfortable with your provider, it may help to find someone you connect with and feel understands your concerns. That relationship can make a major difference in getting consistent care.
Are there newer technologies or innovations in diabetes care that people should know about?
One of the biggest advances has been continuous glucose monitors, or CGMs. These small wearable devices track blood sugar levels in real time and have really changed diabetes care over the past decade.
For providers, CGMs give a much clearer picture of blood sugar patterns throughout the day. For patients, they provide immediate feedback about how food, exercise, and other daily habits affect blood sugar levels.
Someone may notice that certain foods cause major spikes while certain exercises lower their blood sugar. That real-time information helps people make healthier decisions and improve blood sugar control. Research shows these technologies can significantly improve outcomes.
What daily habits or preventative measures can reduce the risk of complications or even amputation?
The biggest thing is controlling your diabetes. A lot of people automatically think diabetes will lead to amputations, but research shows the risk is much lower when diabetes is well managed.
That means taking medications as prescribed, making dietary changes, and working to keep your A1C below 7. Managing high blood pressure and high cholesterol is also important because both contribute to circulation problems.
People should also inspect their feet every day, especially if they’ve already lost sensation. Some patients injure their feet without realizing it because they can’t feel the damage. Catching wounds early is critical. Good foot hygiene also plays a major role in prevention.
Are there any common misconceptions about diabetes that stand out to you in your clinical work with Black patients?
One major misconception is that diabetes medications cause complications like kidney failure or amputations. In reality, poorly controlled diabetes causes those complications — not the medications used to treat it.
Those misconceptions sometimes cause patients to avoid medications or stop taking them altogether. Another issue is that some people believe diet and exercise alone should always control diabetes. While lifestyle changes are important, some patients have severe diabetes that also requires medication.
Needing medication is not a personal failure. Sometimes diet and exercise alone are simply not enough, and medication is necessary to prevent serious complications.
This article is supported by the California Health Care Foundation (CHCF). Visit www.chcf.org
Community
How Four Black Women Bosses Define Wellness
MINNESOTA SPOKESMAN-RECORDER — Four Black women leaders in Minnesota discussed their definitions and practices of wellness. Reverend Joan Austin of Endure Women’s Ministries, Kelsey Joson of InControl, Dr. Ayanna Rakhu of Sankofa Swim International, and arts leader Serena Wright shared their perspectives on what wellness means across their diverse fields.

What Wellness Really Means: Four Black Women Leaders Share Their Practice
Contributing writer Tiffany Johnson talks with four Black women leaders in Minnesota, Reverend Joan Austin of Endure Women’s Ministries, Kelsey Joson of InControl, Dr. Ayanna Rakhu of Sankofa Swim International, and arts leader Serena Wright, about what wellness means across their very different fields. Their answers reveal common threads: protecting daily rituals, finding movement in small joys, and building community that tells the truth with love.
When you hear the word wellness, what comes to mind?
I posed that question to four Black women leaders across sectors in Minnesota: Reverend Joan Austin, founder of Endure Women’s Ministries, a nonprofit supporting women in ministry; Kelsey Joson, founder and CEO of InControl, a wellness hub for adults with disabilities; Dr. Ayanna Rakhu, founder and CEO of Sankofa Swim International, promoting healing for Black and brown bodies through water; and Serena Wright, arts leader and former director in the University of Minnesota’s Office of the Vice Provost for Faculty and Academic Affairs.
I invited each of them to share her perspective on what wellness means and how it shapes different areas of life. What emerged was a reservoir of wisdom, revealing the many ways wellness takes root, and the many ways these women have built their own leadership around it.


Reverend Austin has served as an ordained minister for more than 25 years, and for the past decade she’s run her own nonprofit. “To me, wellness means being well-rounded spiritually, emotionally, mentally and physically. It’s about nurturing each of those aspects of ourselves as we navigate the different experiences and challenges of life,” she said.
“I was at a point where I wanted to give up in ministry, and during prayer, the Lord told me not to give up. He said ‘He needed me to endure,’ and that’s where the name came from.” The name is also an acronym: Equipped, Nurtured, Devoted, United, Renewed and Empowered.

Joson, founder of InControl, has built her career around others’ wellness. “When I hear wellness, what comes to mind is how someone takes care of their body, and not just physically. Wellness was never meant to be one dimensional. It is everything that goes into being a whole human being, the mental piece, the emotional piece, the spiritual piece, all working together to create a firm foundation,” she said.
“InControl is devoted to solving the quality of life crisis for adults with intellectual and developmental disabilities across Minnesota. We provide in-home coaching focused on physical health, nutrition and social emotional wellbeing, meeting clients exactly where they are and helping them build real agency and independence in their own lives.”
Dr. Rakhu leads Sankofa Swim International and serves on the board of V3 Sports, a wellness hub in North Minneapolis, teaching communities from Minnesota to Grenada. “When I hear the word wellness, I picture a set of scales,” she said. “Sometimes one side is heavier than the other, and sometimes they’re perfectly aligned. But the scales are always adjusting. That’s how I think about wellness.”

It’s no coincidence that Rakhu’s specialty exists in the world of water, where balance is essential for survival. She’s passionate about restoring healing in the Black community around its historic relationship with water, challenging stereotypes about Black people and swimming while acknowledging the historical trauma of the transatlantic slave trade and the African diaspora.
“I describe my work as liberation work because I believe healing our relationship with water is liberating,” she said. “The communities I serve are Black people and people of African descent. I’m especially concerned about that relationship. That’s where my work lies.”
Wright, a leader in Minnesota’s arts and education community, finds sanctuary in nature. “Nature has always been a part of who I am. I literally take the time to look at a leaf, because that brings me to life.” Her connection to nature feels fitting given her recent recognition at Flowers Now!: A Celebration of Black Elders of the Arts Community, presented by the Givens Collection of African American Literature in May 2026.

“Wellness is a body, mind and spirit connection,” Wright said. “It’s checking in with myself first, being willing to ask questions, seeking honest feedback and pushing through discomfort. I don’t want to be paralyzed by fear, because that’s how I continue to grow.”
Though Wright recently retired from her longstanding role at the University of Minnesota, she doesn’t see it as an ending, but as “a reset,” continuing part-time at the university while staying deeply engaged in the arts community.
These four women, different in practice, revealed real overlap in how they approach wellness, and leadership.
On community: “You don’t need people tearing you down. You need people who will tell you the truth with love,” Wright said.
On showing up over perfection: “I protect my mornings as time for myself first, before I give my attention to anything else,” Joson said.
On movement: “I really love to roller skate. It reminds me of my capability, reminds me of my joy,” Rakhu said. “Wellness doesn’t have to look like a gym. Movement can be the smallest things we do every day,” Wright added.
On where to start: “Start with prayer, because I know God will lead, guide and direct,” Austin said. Rakhu suggested something simpler: “Make a list. It gets things out of your head and into this world of manifestation.” Wright summed it up: “Wellness isn’t about taking one big step. It’s about the little things you do every day.”
Wellness looks different for everyone, but these women point to one universal truth: caring for ourselves allows us to better care for others. By investing in their own physical, emotional, mental and spiritual health, they’ve become stronger leaders, building lasting impact in the communities they serve.
To learn more, visit Endure Women’s Ministries at endurewomensministries.org, InControl at incontrolmn.com, or Sankofa Swim International at sankofaswim.com.
Tiffany Johnson is a contributing writer for the Minnesota Spokesman-Recorder. She welcomes reader responses at tjohnson@spokesman-recorder.com.
Your Might Also Like
Tiffany Nicole Johnson
Tiffany Nicole Johnson is a marketer, writer and musician based in Minneapolis. Tiffany is a contributing writer for the Minnesota Spokesman-Recorder. She is also the associate director of marketing at… More by Tiffany Nicole Johnson
Based on reporting by Minnesota Spokesman-Recorder.

WORK FROM HOME
Home-based business with potential monthly income of $10K+ per month. A proven training system and website provided to maximize business effectiveness. Perfect job to earn side and primary income. Contact Lynne for more details: Lynne4npusa@gmail.com 800-334-0540
![]()

From Disparity Study to Solutions: Oakland Coalition and Mayor Barbara Lee Renew Commitment to Reform City Contracting

The Congressional Seat That Black History Built (florida’s 20th District)

COMMENTARY: The Two July 4ths: Which Did You Celebrate?

COMMUNITY: What Trump’s Presidency Means for Black Economic Mobility

Trump Administration Shelves Harriet Tubman $20 Bill Plan

COMMENTARY: The Basis of Freedom: Reclaiming Land as an Act of Liberation

Justice and Childhood

Standing Room Only in Raleigh with Leader Sydney Batch and Stacey Abrams

Looking at My Top 10 Black MLB Players List

Preventing Amputation: A Doctor’s Guide for Diabetes Patients

How Four Black Women Bosses Define Wellness

New Minneapolis Mural Imagines Black and Indigenous Futures Among the Stars

Kotelemla Bolinga: a Soundtrack for Resistance and Love

St. Louis Cardinals Outfielder Jordan Walker Claims Franchise’s First Home Run Derby Crown

California’s Unhoused Seniors: a Crisis Within the State’s Homelessness Crisis

After 10-Year Wait, Fillmore Heritage Center Reopens in San Francisco

Oakland Post: Week of June 3 – 9, 2026


Oakland Post: Week of June 17 – 23, 2026

Oakland Post: Week of June 10 – 16, 2026

COMMENTARY: Black Music is the Sound of Black Freedom: Let Us Reclaim Both This Juneteenth

Oakland Director Boots Dazzles Once Again in ‘I Love Boosters’

Sale of Coliseum to African American Developers Moves Toward Completion

2026 World Cup is Here and Atlanta is Ready For It

IN MEMORIAM: Oakland Dance Legend Reginald Ray-Savage, 67

UC Berkeley Named Top Public University in the U.S. and No. 7 in the World by ‘U.S. News’

Ferry Fares to Increase July 1 as Ridership Hits Record Highs

5 Cleveland Police Officers Injured, Gunfire Erupts During East Side Pursuit

A Long Time Coming: School District Kicks Off Massive $97 Million Renovation of West Oakland’s McClymonds High School

Oakland Museum Presents Landmark Retrospective Celebrating Beloved Bay Area Artist Mildred Howard

The Conversation With Al McFarlane 6/23/26

Media Monday 6/22/26

LIVE! ASK ALMA! — TUES. 6.23.26 7PM EST

Car Buying Secrets: 4 Hidden Checks Before You Sign!

Is This 550 HP Charger Worth YOUR Money? AutoNetwork Review

Celebrating Juneteenth – Frederick Douglass on education and resistance

LIVE! — ASK ALMA! — TUES. 6.19.26 7PM EST

Hyundai Ioniq 5 Parking, Safety, and 360 View #shorts

2025 Ioniq 5 New Wiper & Powerful Performance! #shorts

Electric SUV Range: Is 259 Miles Enough? #shorts

EV Charging: How Fast Can You Charge an Electric Vehicle? #shorts

Biometric Cooling… Messaging Seats…Come on! 2025 Infiniti QX80 Autograph 4WD

Charged Up: Witness the Magic of a Fully Electric Car! #shorts

Range Rover Sport PHEV Included…: See What’s Inside This Luxury SUV! #shorts

Invisible Hood View: Perfect Parking with X-Ray Vision! #shorts
-
 Activism3 weeks ago
Activism3 weeks ago -
 Activism4 weeks ago
Activism4 weeks agoOakland Post: Week of June 17 – 23, 2026
-
 Business4 weeks ago
Business4 weeks agoSale of Coliseum to African American Developers Moves Toward Completion
-
 Arts and Culture3 weeks ago
Arts and Culture3 weeks agoIN MEMORIAM: Oakland Dance Legend Reginald Ray-Savage, 67
-
 Bay Area3 weeks ago
Bay Area3 weeks agoUC Berkeley Named Top Public University in the U.S. and No. 7 in the World by ‘U.S. News’
-
 Alameda County3 weeks ago
Alameda County3 weeks agoFerry Fares to Increase July 1 as Ridership Hits Record Highs
-
 Bay Area3 weeks ago
Bay Area3 weeks agoA Long Time Coming: School District Kicks Off Massive $97 Million Renovation of West Oakland’s McClymonds High School
-
 Activism3 weeks ago
Activism3 weeks agoOakland Museum Presents Landmark Retrospective Celebrating Beloved Bay Area Artist Mildred Howard